OSA Appliance Basic Design 101
By Moses, Tessier, and Pacini
There is a complex interrelationship between head posture, breathing, speech, swallowing, and the position of the teeth in the mouth. Teeth and the dental alveoli lie in a position of balance between the cheeks, lips, and tongue. Ideally, there is nasal breathing; the tongue is in contact with the roof of the mouth at rest and during swallowing. Interventions that disrupt nasal breathing cause opening of lips, low tongue position, head forward posture, and malocclusions. Protruding the tongue affects oropharyngeal dilation and decreases airway resistance. Retruding the tongue increases oropharyngeal resistance.
Obstructive sleep apnea (OSA) only occurs during sleep and is created by either the tongue or the soft palate or both together collapsing on the back of the airway and obstructing airflow.
An apneic event is defined as an 80% – 100% reduction in airflow for a minimum duration of 10 seconds but can be for much longer.
Hypopnea is a 50-80% restriction of airflow for a minimum of 10 seconds with oxygen desaturation.
The Apnea-Hypopnea Index (AHI) refers to the number of apneas and hypopneas occurring per hour.
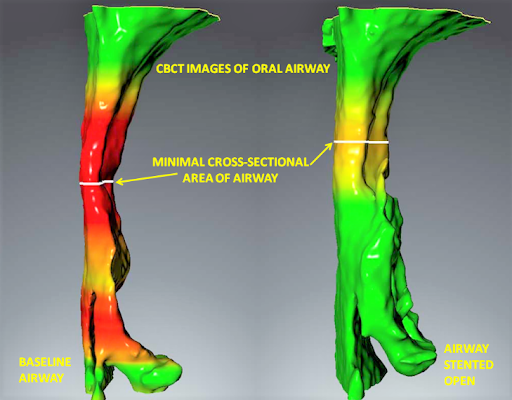
FIGURE 1. A software rendering of a cone-beam image the airway of an apnea patient without an oral appliance on the left and the same patient with a successful oral appliance in position on the right.
The collapse can be caused by muscle flaccidity, negative airway pressure due to increased airway resistance, or a combination of both muscle flaccidity and negative airway pressure in the pharynx. OSA can have severe, morbid pathological consequences including death. Intraoral appliances for the treatment of Obstructive Sleep Apnea (OSA) should function to allow proper physiological tongue positioning and optimal oropharyngeal dilation and stenting.
This article identifies those known, recognized anatomic characteristics of the head, neck, mouth, nose, and throat necessary for optimal physiological function of human beings, and evaluates how they relate to existing intraoral appliances used to treat OSA.
How The Oral Appliance Treats OSA
An ideal prosthetic device properly positioned entirely in the mouth between the dental arches during sleep affects a multi-dimensional neuromuscular dilation in the shape of the oropharynx, a flexible anatomic structure, located downstream and behind the mouth. This dilation and stenting lasts as long as the device remains in the mouth unless mandibular movement occurs causing a change in the airway’s shape.




Mandibular Movement During Sleep Changes the Shape of the Oropharynx
Removal of the device does not bring about an apneic event but increases the susceptibility of the airway to collapse.
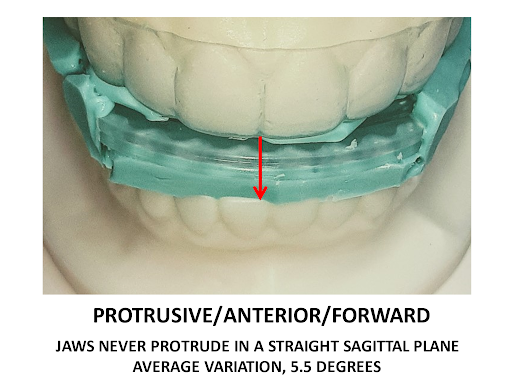
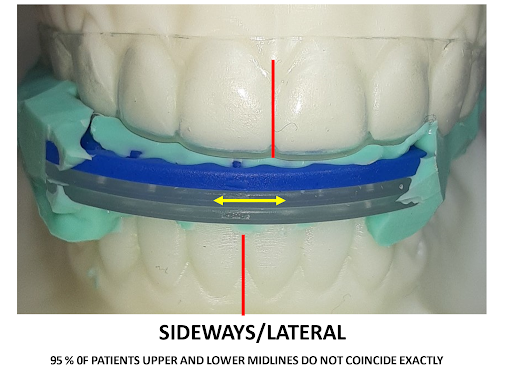
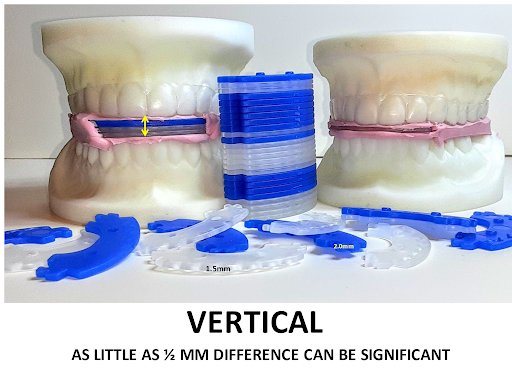
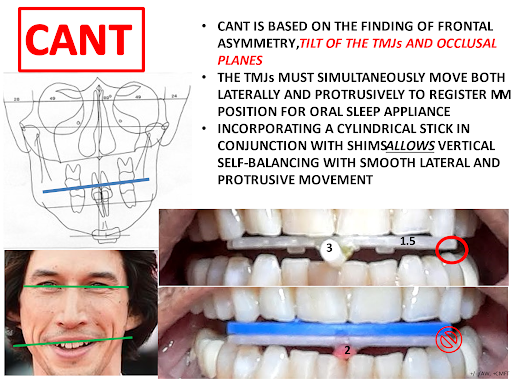
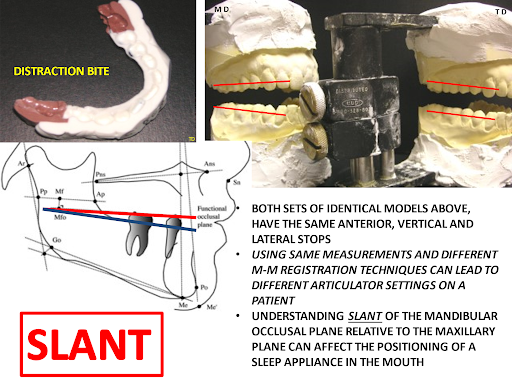
There are at least five dimensional factors that must be considered in determining dental arch positioning for an oral sleep appliance.



With All Moses Sleep Appliances Stable Jaw Position During Sleep and Stable Oral Airway Stenting
In addition, the hormone melatonin is produced at night. A small pineal gland (also called the pineal gland) located in the center of the brain is responsible for its production. Despite the fact that it weighs only one gram, it regulates many processes in our body. For example, during the day it is responsible for the production of seratonin, the hormone of happiness, and at night, respectively, for the production of melatonin.
The hormone melatonin is responsible for the restoration of the psyche, cardiovascular and immune systems, and also with its help, rejuvenating processes take place in the body. The most active production of melatonin occurs between 24:00 pm and 02:00 am.
For its normal production, you need to sleep in absolute darkness, so it is impossible to make up for the lack of this hormone with a daytime sleep. The largest amount of melatonin is produced in infants and, unfortunately, decreases with age.
Oral Sleep Appliances, in order to affect the airway dilation, increase inter-arch volumetric dimension, increasing volume of space for the tongue, stimulate and train protrusive tongue reflexes, correct dysphagias, and alter the position of the hyoid bone relative to the mandible. Achieving the optimal position of neurophysiological dilation and stenting is very complex, multi-dimensional and not easily accomplished. Most oral sleep appliances have built-in mechanical adjustment mechanisms, usually screws, hinges, tubes, straps, springs, and rubber bands. This does allow for post-insertion adjustment, thus the overwhelming majority of sleep appliances are not titrated before insertion the big problem with this protocol is that it is illogical and not science-based.
All sleep appliances with built-in adjustment mechanisms are only capable of movement in one dimension and do not replicate the biological movement of human jaws, which move both multidimensionally and asymmetrically.
A fundamental design principle is, “The more room created for the tongue in the mouth, the less likely it is to collapse on the airway during sleep.” In ideal function, an intraoral sleep appliance facilitates the most tongue space possible in the mouth. It should allow the most anterior possible tongue position, which means that the tip of the tongue can touch the closed lips. Ideal function necessitates that an appliance is positioned within the normal envelop of movement of the TMJ, creating no jaw pain or discomfort. There is no normal function in which the tongue is positioned outside the lips. An excellent oral sleep appliance facilitates tongue positioning in contact with the hard and soft palate at rest and not having a component of the appliance situated to displace the tongue. A well-designed oral sleep appliance allows the lips to stay together with the patient breathing through the nose. Intraoral sleep appliances are much more likely to control OSA in nose breathers than in mouth breathers.
The ideal maxillo-mandibular position is based on certain postural axioms and neurophysiological principles. In human beings, the essential function of the back and neck is to support the head in an upright posture. In the upright human posture, isometric balance is the least stressful position for supporting the head on the spinal column. Tongue positioned in the roof of the mouth (largest oral airway), lips together (necessitating nose breathing), teeth apart, and patient standing up as straight as possible (isometric balance) are necessary axioms for registering a maxillo-mandibular position that creates optimal tongue space.
Summary Successful Design Criteria For OSA Sleep Appliance:
Integrating the biomechanical elements of the human oropharyngeal system into the design and function of intraoral sleep appliances to optimize overall system performance defines ERGONOMICS.
- The larger the space created for the tongue the less likely it is to collapse on the airway during sleep
- Tongue position in the appliance is the same as that of the largest patent airway during wakefulness
- The device must allow comfortable closure of the lips (otherwise oral breathing would occur)
- Jaw (TMJ) positions in the appliance must not cause pathologic TMJ damage, such as a displaced disk
- The tongue should not be restricted from contact with closed lips due to the presence of an anterior adjustment mechanism
- The tongue must be able to position itself flat against the palate (not prevented or restricted by structural material of the oral appliance)
- The structure that allows tongue positioning flush against palatal rugae stimulates nasal patency
- The appliance should not impede nasal breathing
- The appliance should restrict collapse of the tongue on pharynx during sleep
- The appliance should increase resting muscle tonus during sleep
- Oral sleep appliance should increase the volume of airflow through the pharynx and larynx during sleep (oral airway dilation/stenting)
- Facilitate protrusive tongue reflexes by tactile stimulation
- Not decrease the volume of airflow (by stuffing tongue in the throat)
- Patient’s speech with the appliance in place should be understandable
- The device should be durable, adjustable, cleanable
- The tongue must be naturally positioned inside the mouth, not beyond the lips during sleep (such as with tongue retaining devices TRDs)
- Establish optimal initial registration of Maxillo-Mandibular jaw position assuring little or no TMJ dysfunction, face pain, and decreased neurological clutter during treatment.
Titration Before Insertion Eliminates the Need for Mechanical Adjustment Device

Contact Teresa at Modern Dental for a Starter Kit (773)631-8888
Not just an unbelievable low price it’s better because:
- Optimal oral airway stenting
- Stable support of oral airway
- Five-dimensional positioning
- Scientific registration Technigue
- Ergonomic Design
- Custom Made
For more information use the button below.
Characteristics of Oral Sleep Appliances That Do NOT Meet the Design Criteria Discussed in This Article:
- Adjustment mechanisms that only adjust in one dimension do not replicate human biological jaw movement (out-dated, obsolute, deficient, flawed science)
- Screws, tubes, hinges, rubber bands and straps that only adjust in one dimension are not ergonomic, unidirectional and not custom to the patient
- Patient is unable to position their tongue anteriorly to contact closed lips
Bulk of material obstructs natural tongue position against palate - Tongue movement so limited patient cannot speak with appliance in place
- Bulky material does not increase or possibly decreases volume of space for tongue.
- Tongue cannot be positioned for sleep in a position within the normal envelop of physiological movement (such as with TRDs)
- Metal clasps, because they cause tooth movement
- Too much vertical for patient to comfortably close lips with appliance in place
- Adjustment mechanisms that cannot replicate three dimensional biological jaw movement
- Mechanical adjustment mechanisms cause lip protrusion and discomfort
- Parts that touch dorsal surface of the tongue cause gagging
About the Author

Dr. Moses held a faculty appointment as an assistant professor of Rush University Medical School in the Department of Sleep Disorders. He is a Diplomate of both the American Board of Craniofacial Pain and the American Board of Dental Sleep Medicine.
He honorably served for two years in the United States Air Force. He then practiced clinical dentistry at his office in the Willis Tower in Chicago, IL until he retired in 2015. Dr. Moses held a faculty appointment as an assistant professor at Rush University College of Medicine in the Department of Sleep Disorders and was a dental consultant in the Department of Sleep Disorders/Neurology at Northwestern University Medical School. He has also taught in 12 different countries. Additionally, Dr. Moses held an appointment in the Dental Products Panel of the United States Food and Drug Administration for more than 10 years.